Introduction to Zepbound Eye Problems: Spine-Chilling Side Effects
Welcome to an authoritative analysis of the Zepbound Eye Problems. Zepbound (tirzepatide) has quickly become one of the most discussed prescription options for chronic weight management. It is effective, it is widely prescribed, and it is increasingly used by patients who also live with type 2 diabetes risk factors. With that momentum comes a predictable question, asked in clinics and in online patient communities every day.
What about Zepbound eye problems?
The responsible answer is precise: tirzepatide is not “an eye drug,” but it can influence biological systems that affect the eyes, particularly through rapid glycemic change, dehydration, blood pressure shifts, and diabetes related retinal vulnerability. In a small subset of patients, visual symptoms can signal urgent conditions that require immediate evaluation, regardless of whether Zepbound is the direct cause.
This article explains what is known, what is plausible, what is rare but serious, and what you should do if vision changes occur.
If you were prescribed Zepbound and took it as directed and suffered Zepbound and NAION, Zepbound vision loss or other Zepbound eye problems, contact Zepbound Vision Loss Lawyer Timothy L. Miles today. You could be eligible for a Zepbound vision loss lawsuit and potentially entitled to substantial compensation. (855) 846–6529 or [email protected].
What Zepbound Is, and Why the Eyes Can Be Affected Indirectly
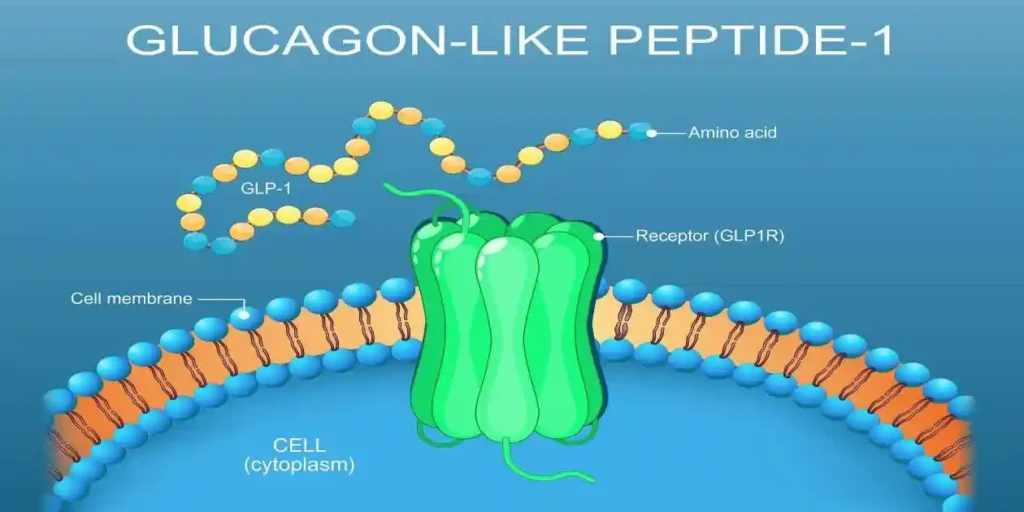
Zepbound is tirzepatide, a dual incretin agonist that activates GIP (glucose dependent insulinotropic polypeptide) and GLP 1 (glucagon like peptide 1) receptors. This can lead to:
- Reduced appetite and caloric intake
- Slower gastric emptying
- Improved insulin sensitivity
- Lower blood glucose (especially in people with diabetes or prediabetes)
- Meaningful and sometimes rapid weight loss
From an ophthalmology perspective, the key point is not that tirzepatide targets ocular tissues. The key point is that metabolic changes can change ocular physiology, and in susceptible patients, those changes can unmask or accelerate underlying problems.
The eye is highly vascular. The retina is metabolically demanding. The optic nerve is sensitive to perfusion. Anything that shifts glucose control, hydration status, blood pressure, or vascular tone can change symptoms, even if the medication is not “toxic to the eye” in the classic sense.
The Most Reported “Zepbound Eye Symptoms” Are Often Not Primary Eye Disease
Many Zepbound users who report “eye problems” describe symptoms that can be explained by systemic effects. These issues can be unpleasant and alarming, but they are often reversible with appropriate evaluation and management.
1) Zepbound and Blurry vision (transient)
Blurred vision is one of the most common visual complaints reported by people whose glucose levels change quickly, regardless of the cause. The lens can temporarily change its refractive properties when glucose shifts, leading to:
- Blurry distance vision or near vision
- Fluctuating clarity throughout the day
- New difficulty focusing
Why it matters: If you are diabetic, rapid improvement in glycemic control can sometimes correlate with short term visual fluctuation. You still need evaluation, but the mechanism is often metabolic rather than structural eye damage.
What to do: Document timing, check blood glucose trends if relevant, and schedule an eye exam if blur persists longer than a few days or is accompanied by floaters, flashes, pain, or field loss.
2) Zepbound Dry Eye Syndrome and Irritation
Zepbound commonly causes gastrointestinal side effects such as nausea, vomiting, or reduced intake. Lower fluid intake plus fluid loss can contribute to dehydration, which can worsen:
- Dry eyes
- Burning or grittiness
- Intermittent blurred vision that improves with blinking
- Contact lens intolerance
What to do: Hydration, electrolyte balance if appropriate, preservative free artificial tears, and review of other drying medications (antihistamines, isotretinoin, some antidepressants) can help. Persistent redness, discharge, or photophobia warrants evaluation.

3) Headache related visual disturbance
Some people experience headaches during dose escalation or periods of reduced caloric intake. Headaches can be associated with:
- Light sensitivity
- Temporary visual shimmer
- Migraine aura (zig zags, scotoma, wavy lines)
Important distinction: Migraine aura is usually temporary and bilateral in visual perception, but new aura symptoms after age 40, prolonged aura, or aura with neurological deficits requires medical review.
If you were prescribed Zepbound and took it as directed and suffered Zepbound and NAION, Zepbound vision loss or other Zepbound eye problems, contact Zepbound Vision Loss Lawyer Timothy L. Miles today. You could be eligible for a Zepbound vision loss lawsuit and potentially entitled to substantial compensation. (855) 846–6529 or [email protected].
The “Spine-Chilling” Category: Symptoms That Should Never Be Ignored
If you take nothing else from this article, take this section seriously. Certain symptoms are medical emergencies because delayed treatment can mean permanent vision loss.
Seek emergency care now if you experience:
- Sudden loss of vision in one or both eyes
- A curtain or shadow over your vision
- New flashes of light with many new floaters
- Severe eye pain with redness, headache, and nausea
- Double vision with weakness, facial droop, slurred speech, or confusion
Zepbound might be coincidental in some cases, but your priority is immediate evaluation, not debating causality.
Zepbound, Diabetes, and the Retina: The Most Clinically Relevant Link
The most important real world context is this: many Zepbound patients have type 2 diabetes, prediabetes, or longstanding insulin resistance. In these populations, the retina may already be vulnerable.
Zepbound and Diabetic retinopathy (DR) basics
Diabetic retinopathy is microvascular damage to the retina caused by chronic hyperglycemia. It ranges from mild non proliferative disease to proliferative retinopathy and diabetic macular edema.
Symptoms can include:
- Zepbound and Blurry vision
- Distorted central vision (macular edema)
- Zepbound and Eye Floaters
- Progressive vision loss
- Sometimes no symptoms until advanced disease
Why medication driven glucose improvement matters
A well known phenomenon in diabetes care is early worsening of diabetic retinopathy when glucose control improves rapidly. This has been described historically with intensive insulin therapy and has been discussed in relation to incretin based therapies as well, mainly as a risk consideration in patients with pre existing retinopathy and large, rapid A1C reductions.
Core concept: Long term glucose control reduces retinopathy progression, but a rapid drop in A1C over a short period can be associated with short term worsening in some high risk patients.
That does not mean Zepbound “causes retinopathy” in the way an ocular toxin would. It means Zepbound can be part of a treatment plan that changes glucose fast enough to reveal a known risk dynamic.

Who is higher risk?
- Patients with pre existing diabetic retinopathy
- Patients with poor baseline glycemic control (high A1C) who improve quickly
- Patients with diabetic macular edema history
- Patients who have not had a dilated retinal exam in years
Practical recommendation (risk based)
If you have diabetes and are starting Zepbound, the proactive governance approach is simple:
- Get a baseline dilated eye exam if not current.
- Communicate your A1C trajectory to both your prescriber and your eye clinician.
- Report new floaters, distortion, or field loss immediately.
- If your clinician is targeting an aggressive A1C reduction, ask about pace and monitoring, especially if you already have retinopathy.
Can Zepbound Cause Optic Nerve Problems?
Patients often worry about the optic nerve because optic neuropathies can be sudden and devastating. There is no widely established mechanism that tirzepatide directly damages the optic nerve in typical use. However, several indirect pathways can contribute to optic nerve related symptoms in the general medical setting, including in patients taking weight loss medications.
Potential indirect contributors (not proof of causation)
- Hypotension or volume depletion: Reduced perfusion can stress vulnerable optic nerves in susceptible individuals.
- Sleep apnea changes: Weight loss can improve sleep apnea over time, but during transitions, fatigue patterns and blood pressure patterns can shift.
- Nutritional compromise: Significant appetite reduction without adequate nutrition can contribute to deficiencies (rare, but relevant in restrictive intake patterns).
The symptom pattern that requires urgent evaluation
- Sudden painless vision loss (especially one eye)
- Loss of color saturation
- Visual field defect
- Eye pain with movement (more typical of optic neuritis)
If any of these occur, treat it as urgent, regardless of your medication list.
Retinal Detachment, Tears, Flashes, and Zepbound and Eye Floaters: Where Patients Get Confused
Online discussions frequently mix common benign floaters with serious retinal events.
Common floaters
Many adults have floaters from normal vitreous aging. They can become more noticeable during times of stress, dehydration, or increased attention to visual sensations.
Dangerous pattern
- Sudden shower of floaters
- Flashes of light
- Curtain like shadow
- Peripheral vision loss
These symptoms can indicate retinal tear or detachment, which requires same day evaluation. There is no clear evidence that Zepbound directly causes retinal detachment, but the correct clinical response is the same either way.
Angle Closure Glaucoma: Rare, Severe, and Time Sensitive
Acute angle closure glaucoma presents dramatically and is an emergency. It is not a typical side effect of tirzepatide, but it is one of the “never miss” diagnoses whenever a patient reports severe eye pain and blurred vision.
Classic symptoms:
- Severe eye pain
- Red eye
- Headache
- Halos around lights
- Nausea or vomiting
- Sudden blurred vision
Because nausea and vomiting can also occur from Zepbound itself, patients sometimes misattribute the entire cluster to gastrointestinal side effects and delay care. That is the danger.
If severe eye pain and red eye occur, do not wait it out.
If you were prescribed Zepbound and took it as directed and suffered Zepbound and NAION, Zepbound vision loss or other Zepbound eye problems, contact Zepbound Vision Loss Lawyer Timothy L. Miles today. You could be eligible for a Zepbound vision loss lawsuit and potentially entitled to substantial compensation. (855) 846–6529 or [email protected].
Zepbound and NAION
Clinical Features
Symptoms:
NAION generally manifests as a sudden, painless loss of vision in one eye. Although uncommon, both eyes may be affected, particularly in situations involving major fluctuations in blood pressure such as after surgery, during hemodialysis, or following significant blood loss. Most patients do not experience eye discomfort, headache, or pain around the eye; however, about 10% report these symptoms. If pain is present alongside vision loss, it is important to consider other potential causes.
Signs:
Vision impairment in NAION is usually less profound than what is seen in arteritic anterior ischemic optic neuropathy (AAION). Complete loss of light perception is rare with NAION and should raise suspicion for AAION if encountered. At the initial evaluation, roughly half of individuals with NAION have visual acuity better than 20/64, and two-thirds maintain vision better than 20/200. Some patients may even retain normal visual acuity.
The most frequent visual field abnormality is loss of the lower half of the visual field (inferior altitudinal defect), though other patterns such as inferior nasal deficits or central, cecocentral, and arcuate scotomas can also occur.
Color vision disturbances (dyschromatopsia) and a relative afferent pupillary defect may also be observed. In NAION, the severity of color vision loss generally parallels the degree of visual acuity reduction. This contrasts with optic neuritis, where color vision loss tends to be disproportionately severe compared to the level of visual acuity.
Fundus Findings:
On examination of the back of the eye (fundus), there is often swelling of the optic nerve head that can be either widespread or localized to one segment. Additional findings may include small peripapillary hemorrhages (splinter or flame-shaped), dilated and telangiectatic capillaries near the disc, and narrowing of nearby retinal arterioles. Cotton-wool spots are rarely seen; their presence should prompt consideration of AAION. The unaffected eye may display structural features indicating increased risk for developing NAION in the future.
What About “Eye Pressure,” “Eye Strain,” and Screen Blurriness?
A large number of patient reports fall into a non specific category:
- “My eyes feel pressured.”
- “I have eye strain.”
- “My screen looks blurry.”
These can stem from:
- Zepbound Dry eye syndrome
- Uncorrected refractive error (your prescription may be slightly off)
- Glucose related lens changes
- Migraine physiology
- Anxiety and heightened symptom monitoring during new medication starts
The correct approach is structured and boring, which is good in medicine:
- Check hydration and sleep.
- Confirm you are eating adequately and not skipping protein and micronutrients.
- Review glucose trends if diabetic.
- Get an optometry or ophthalmology exam if symptoms persist beyond 1 to 2 weeks or worsen.

A Practical Symptom Checklist: When to Watch vs When to Act
Monitor closely and schedule a routine eye visit if:
- Mild intermittent blur that comes and goes
- Dryness, burning, gritty sensation
- Mild headache with transient visual sensitivity
- Symptoms correlate with dehydration or long screen sessions
Call your clinician promptly (same week) if:
- Persistent blurred vision for more than a few days
- New distortion (straight lines look wavy)
- Increasing floaters without flashes
- Vision changes after a dose increase that do not stabilize
Seek urgent or emergency evaluation now if:
- Sudden vision loss
- Curtain or shadow
- Flashes with a sudden shower of floaters
- Severe eye pain or a red eye with nausea
- Double vision with neurological symptoms
How to Reduce Risk Proactively (Without Panic)
Forward thinking medication use is not about fear. It is about systems, monitoring, and early detection.
1) Do not start Zepbound “blind” if you have diabetes
If you have type 2 diabetes, or long standing prediabetes with high A1C history, treat eye monitoring as part of the plan.
- Baseline dilated retinal exam
- Follow up schedule based on your retinopathy status
- Clear thresholds for urgent reporting
2) Avoid dehydration, especially during titration
Dehydration is a common amplifier of eye discomfort.
- Aim for steady fluid intake
- Replace electrolytes if advised by your clinician
- Manage nausea early so you can maintain intake
3) Stabilize glycemic improvements when clinically appropriate
Improving glucose is good. Improving too fast in the presence of advanced retinopathy can be risky. The correct pace is individualized and should be set by your treating clinician.
4) Maintain nutrition while losing weight
Rapid weight loss without adequate protein and micronutrients can increase fatigue, dryness, and headaches.
A practical baseline to discuss with your clinician or dietitian:
- Sufficient protein
- Adequate omega 3 intake (if appropriate)
- Iron, B12, folate status if intake is low or fatigue is significant
5) Keep your medication list coordinated
If you take diuretics, antihypertensives, migraine medications, antihistamines, or diabetes agents, interactions can shape symptoms like hypotension, dehydration, and visual fluctuation. Coordination prevents unforced errors.
What to Tell Your Doctor (Use This Script)
If you are experiencing eye symptoms on Zepbound, clarity helps your clinician triage correctly. Use a structured description:
- Onset: sudden or gradual, date and time
- Laterality: one eye or both
- Symptom type: blur, distortion, flashes, floaters, pain, redness, double vision
- Severity: mild, moderate, severe
- Associated factors: headache, nausea, dehydration, low blood sugar symptoms
- Recent changes: dose escalation, rapid weight loss, recent A1C drop, blood pressure changes
- Past ocular history: retinopathy, glaucoma, macular edema, high myopia, previous retinal tear
This is governance at the patient level. The goal is not to self diagnose. The goal is to communicate risk efficiently so the right care happens fast.
If you were prescribed Zepbound and took it as directed and suffered Zepbound and NAION, Zepbound vision loss or other Zepbound eye problems, contact Zepbound Vision Loss Lawyer Timothy L. Miles today. You could be eligible for a Zepbound vision loss lawsuit and potentially entitled to substantial compensation. (855) 846–6529 or [email protected].
Frequently Asked Questions about Zepbound Eye Problems
What about Zepbound blindness?
There is no credible basis to claim that Zepbound commonly “causes blindness.” However, serious eye conditions can occur in the population, and diabetes related retinal disease can progress. Any sudden severe symptoms require urgent evaluation.
Can Zepbound worsen diabetic retinopathy?
In patients with diabetes, rapid improvement in glucose control has been associated with short term worsening of retinopathy in certain high risk contexts. The practical approach is baseline screening, paced control when appropriate, and close monitoring if retinopathy already exists.
Why is my Zepbound and blurry vision after starting or increasing the dose?
Common reasons include glucose related refractive shifts, dehydration related dry eye, headaches or migraine physiology, and general adaptation during titration. Persistent blur should be evaluated to rule out retinal disease.
Should I stop the medication if I notice Zepbound vision problems?
Do not make unilateral medication changes based on fear. If symptoms are emergency level, seek emergency care. If symptoms are non emergent but persistent, contact your prescriber promptly and schedule an eye exam. Your clinician will decide whether to pause, adjust dose, or investigate other causes.
Why might Zepbound and dry eye syndrome or eye irritation?
Zepbound can cause gastrointestinal side effects like nausea and vomiting that reduce fluid intake, leading to dehydration. Dehydration worsens dry eyes, causing symptoms such as burning, grittiness, intermittent blurred vision that improves with blinking, and contact lens intolerance. Managing hydration and using preservative-free artificial tears can alleviate these symptoms. Persistent redness or photophobia requires medical evaluation.
Are headaches and visual disturbances linked to Zepbound use?
Some individuals on Zepbound may experience headaches during dose escalation or periods of reduced caloric intake. These headaches can be associated with light sensitivity and temporary visual disturbances like migraine aura (zig zags, wavy lines). While migraine aura is typically temporary and bilateral, new aura symptoms after age 40 or those accompanied by neurological deficits warrant immediate medical review.
What Zepbound eye symptoms require urgent medical attention?
Certain symptoms are medical emergencies regardless of Zepbound use. Seek immediate care if you experience sudden vision loss in one or both eyes; a curtain or shadow over your vision; new flashes of light with many floaters; severe eye pain with redness, headache, and nausea; or double vision accompanied by weakness, facial droop, slurred speech, or confusion. Prompt evaluation is critical to prevent permanent vision loss.
How does Zepbound relate to diabetic retinopathy risk?
Many patients taking Zepbound have type 2 diabetes or prediabetes, conditions that can make the retina vulnerable to damage known as diabetic retinopathy (DR). DR involves microvascular damage from chronic high blood sugar and can cause blurry vision, distorted central vision due to macular edema, floaters, progressive vision loss, or sometimes no symptoms until advanced stages. Monitoring retinal health during treatment is essential.
The Bottom Line
Zepbound can be associated with eye related symptoms, most often through indirect pathways such as dehydration, headaches, and rapid metabolic change. The most clinically important risk context is diabetes and diabetic retinopathy, where rapid glycemic improvement can sometimes correlate with short term retinal worsening in susceptible patients.
The correct response is not panic. The correct response is governance:
- Baseline eye screening when risk exists
- Clear symptom thresholds for urgent care
- Hydration and nutrition discipline during titration
- Coordinated management between prescriber and eye clinician
If you develop sudden vision loss, flashes with a surge of floaters, a curtain over vision, or severe eye pain with redness, treat it as urgent. The fastest path to safety is immediate evaluation, not speculation.
If You Suffered from Zepbound Eye Issues or Other Zepboound Vision Problems, Contact Zepbound Vision Loss Lawyer Timothy L. Miles Today
If you were prescribed Zepbound and took it as directed and suffered Zepbound and NAION, Zepbound vision loss or other Zepbound eye problems, contact Zepbound Vision Loss Lawyer Timothy L. Miles today. You could be eligible for a Zepbound vision loss lawsuit and potentially entitled to substantial compensation. (855) 846–6529 or [email protected].
Timothy L. Miles, Esq.
Law Offices of Timothy L. Miles
Tapestry at Brentwood Town Center
300 Centerview Dr. #247
Mailbox #1091
Brentwood,TN 37027
Phone: (855) Tim-MLaw (855-846-6529)
Email: [email protected]
Website: www.classactionlawyertn.com
Facebook Linkedin Pinterest youtube
![]()